

This article contains affiliate links. If you purchase through our links, we may earn a small commission at no extra cost to you. This does not affect our editorial recommendations.
Quick answer: Perimenopause and anxiety share nearly identical symptoms, but they have different mechanisms, different triggers, and different treatments. The key difference: perimenopause anxiety is hormonally driven, often follows your menstrual cycle, and typically arrives alongside sleep disruption and period changes. Primary anxiety disorder is usually thought-driven and doesn’t track with your cycle. Nearly 40% of women with perimenopause symptoms are diagnosed with anxiety instead, and treated for the wrong thing. This article shows you how to tell the difference, and what to do if you’ve been misdiagnosed.
The anxiety arrived out of nowhere. Not the ordinary kind. Not the big-presentation-tomorrow kind or the something-bad-might-happen kind. The kind that wakes you at 3am on a perfectly normal Tuesday and sits in your chest for no reason you can name. The kind that made you wonder, seriously, if you had developed an anxiety disorder overnight.
And then you went to the doctor. And they said: stress. Maybe burnout. Possibly you need to think about an antidepressant.
Here’s what nobody told you: when women in their late 30s and early 40s try to work out whether they’re dealing with perimenopause vs anxiety, or perimenopause vs burnout, they are asking exactly the right question. Nearly 40% of women who seek care for what turns out to be perimenopause, not anxiety, are misdiagnosed. More than half of them walk out of that appointment with a treatment for anxiety, depression, or panic disorder, instead of the hormonal shift that is actually driving everything they are feeling.
If you are in your late 30s or early 40s, and something has felt deeply, persistently off for the past several months or years (your sleep, your moods, your ability to think clearly, your sense of yourself), this article is for you. Not to diagnose you. But to give you the information your doctor appointment probably didn’t.
We are going to walk through what perimenopause anxiety actually looks like, how it differs from primary anxiety disorder, why the two are so consistently confused, and what you can do right now to start getting real answers instead of real medication for the wrong thing.
40% of women seeking care for perimenopause symptoms are misdiagnosed. More than half treated for anxiety or depression instead.
15% of women felt adequately informed about perimenopause when their symptoms began. Fewer than half had a provider ever raise it.
39% of women prescribed medication for conditions like depression believe they were not appropriately diagnosed.
Something Changed. You’re Not Imagining It.
Before we get into mechanisms and checklists and what to do, let’s start with the thing you actually need to hear first.
What you are experiencing is real. It has a clinical name. And the fact that you have been told it is stress, burnout, anxiety, depression, ‘you have a lot on,’ or ‘you’re too young for that’ does not mean those people were right. It means they were working from an incomplete picture, which is a gap in medical training, not a verdict on your body.
Women in their late 30s and early 40s are the most under-diagnosed group in the perimenopause space. If you’re 38 or 39 and your doctor keeps saying you’re too young, you’re not. The cultural story of menopause (hot flashes at 50, hormones tanking overnight, sudden transition) is medically inaccurate for the majority of women. The real picture is a gradual hormonal shift that, for many women, begins between 35 and 45, with psychological symptoms typically arriving before the physical ones.
The single most important fact in this article: For many women, the first signs of perimenopause are not hot flashes. They are anxiety, mood changes, sleep disruption, and brain fog. These symptoms often arrive years before periods become irregular. And they are almost universally attributed to something else.
A 2025 study published in npj Women’s Health found that psychological symptoms not only precede physical ones in perimenopause. They tend to peak between the ages of 41 and 45. That’s the exact window during which most doctors are still telling women they’re ‘too young’ for any of this to be hormonal.
You are not too young. That isn’t reassurance. It’s the documented clinical range. The late 30s is within the normal onset window for perimenopause. Your doctor’s ‘you’re too young’ is not based on current evidence. It’s based on a model of menopause that was built around a 50-year-old, not you.
Is It Perimenopause or Anxiety? Understanding Why They Look the Same
This is the crux of it. The reason perimenopause anxiety is so consistently misdiagnosed as primary anxiety disorder is that the symptoms are, on the surface, nearly identical. Racing heart. Waking at night. Chest tightness. Irritability. Perimenopause mood swings. Difficulty concentrating. A sense of dread that doesn’t have a clear object.
But the mechanism is completely different. And the mechanism is what determines the treatment. Getting the mechanism wrong means getting the treatment wrong, which is why so many women end up on SSRIs or benzodiazepines that help a little but never quite resolve what they’re actually experiencing.
Is this perimenopause or anxiety? The hormone-neurotransmitter explanation
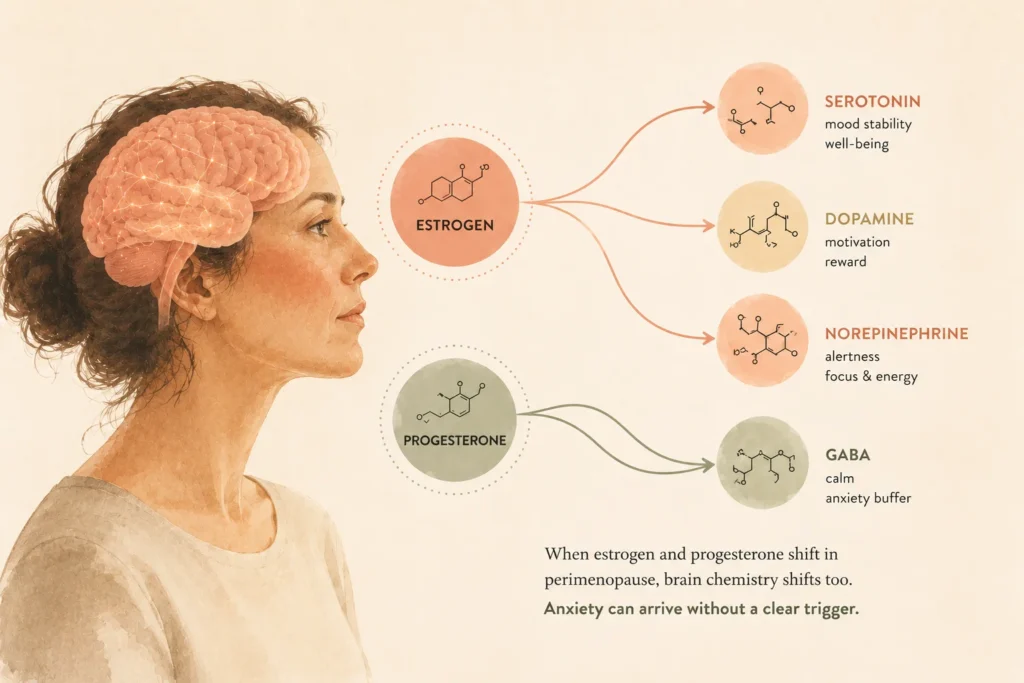
Estrogen is not just a reproductive hormone. It directly regulates serotonin, dopamine, and norepinephrine: the three neurotransmitters that control mood, focus, and the nervous system’s response to threat. When estrogen begins to fluctuate in early perimenopause, these systems fluctuate with it.
This is why perimenopause anxiety often feels different from anxiety you may have experienced earlier in life. It’s not being generated by worried thoughts about specific things. It’s being generated by a body in a different chemical state, and your mind is frantically searching for a reason that doesn’t exist.
Progesterone is the other piece of the hormone imbalance anxiety picture. Progesterone has a natural calming, GABA-agonist effect on the brain. It is often the first hormone to decline in early perimenopause. When progesterone drops, the brain loses a natural anxiety buffer, and the result is an uptick in anxiety, irritability, and sleep disruption that arrives without any obvious trigger.
The 7 overlap symptoms that cause perimenopause misdiagnosis
These are the symptoms that appear in both primary anxiety disorder and perimenopause-driven hormonal change. They are the reason the diagnostic confusion happens, and understanding how they differ in each condition is the key to working out which one you’re actually dealing with.
In primary anxiety: Often linked to worry or rumination — replaying events, anticipating problems.
In perimenopause anxiety: Often without specific thought content. Physiological arousal only: heart pounding, wide awake, no particular worry driving it.
Key differentiator: No anxious thought content alongside the physical arousal strongly suggests hormonal origin.
In primary anxiety: Usually triggered — a specific event, stressor, or accumulated pressure precedes it.
In perimenopause anxiety: Disproportionate or unprompted. Often spikes in the 7-10 days before period, in the luteal phase.
Key differentiator: Cyclical pattern and premenstrual timing points to hormonal cause.
In primary anxiety: Common during or after anxious episodes; typically accompanied by anxious thinking.
In perimenopause anxiety: Can occur at rest, at night, without anxious thought content. Vasomotor in origin.
Key differentiator: Occurring at rest or nocturnally without worried thoughts is a hormonal signal.
In primary anxiety: Present during high-anxiety periods; improves when anxiety reduces.
In perimenopause anxiety: Persistent, baseline-level blunting of focus that doesn’t track with anxiety peaks.
Key differentiator: Constant, non-episodic quality regardless of anxiety state — an estrogen-hippocampus effect.
In primary anxiety: Difficulty falling asleep due to racing thoughts; waking with anxiety content.
In perimenopause anxiety: Often falling asleep fine, then waking between 2-4am without worry content. Progesterone-related.
Key differentiator: Falling asleep normally then waking without anxious thoughts strongly suggests perimenopause.
In primary anxiety: Often situational or has a clear emotional arc. Linked to life circumstances.
In perimenopause anxiety: A flatness or emotional blunting that feels disconnected from circumstances. No obvious trigger.
Key differentiator: Mood that doesn’t track with life events and improves in follicular phase is hormonal.
In primary anxiety: Often accompanies anxiety as nervous-system depletion. Improves with anxiety treatment.
In perimenopause anxiety: Persistent regardless of sleep quality or anxiety state. A ‘bone tired’ quality.
Key differentiator: Persists even on good sleep nights and doesn’t improve with anxiety treatment alone.
The 4 signals that point specifically to hormones, not primary anxiety
Beyond the table above, there are four patterns that, if you recognize them, are disproportionately likely to indicate a hormonal origin rather than a primary mental health condition. They are not diagnostic on their own. But they are meaningful data.
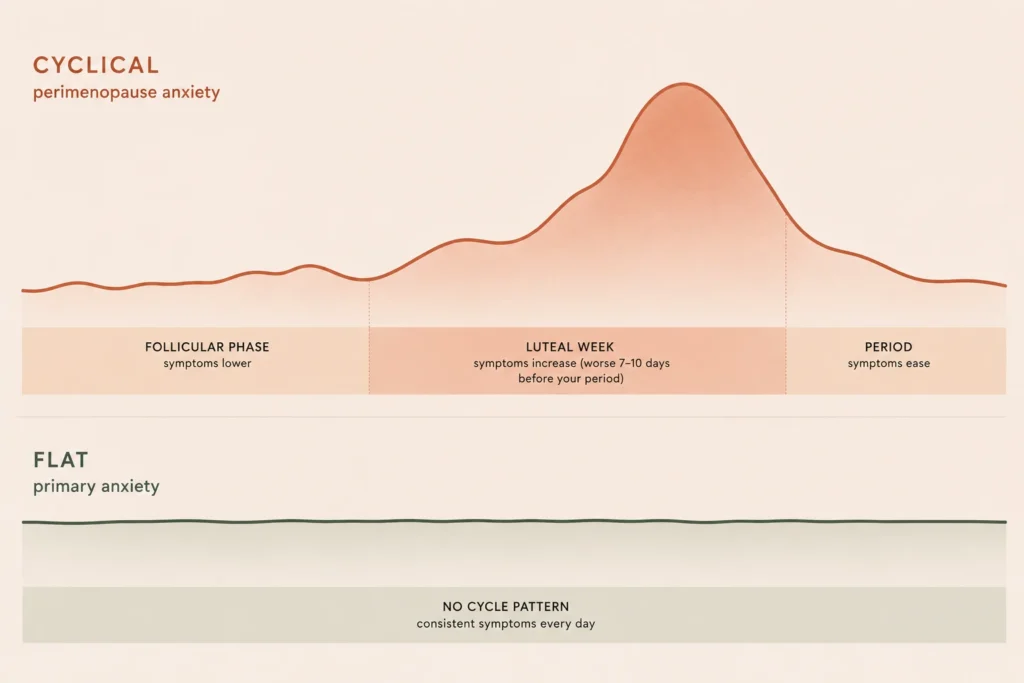
1. Your symptoms are cyclical. They get worse in the 7-10 days before your period, then improve after it starts. This tracks with the luteal phase drop in progesterone and estrogen. Primary anxiety disorder does not usually follow your menstrual cycle.
2. Your periods have changed. Heavier, lighter, closer together, further apart, or less predictable. Period changes are often the first physiological signal of perimenopause, and they frequently arrive alongside the mood and sleep changes, not after them.
3. The anxiety feels physically driven. Not ‘I’m worried about something’ but ‘my body is in a state and my mind is trying to explain it.’ This is the estrogen-serotonin mechanism: the physiological arousal is primary, and the mental interpretation follows.
4. Your symptoms arrived without a clear life trigger. Not a difficult period at work. Not a relationship change. Not a loss. Just: one day things were fine, and then gradually, or suddenly, they weren’t.
Why Doctors Get This Wrong, And Why That’s Not Entirely Their Fault
The misdiagnosis rate is real and documented. But understanding why it happens matters, both so you stop wondering if you’re imagining things, and so you can navigate the next appointment more effectively.
When you walk into your GP’s office and describe anxiety, sleep disruption, and perimenopause mood swings, your doctor runs a reasonable diagnostic process for those symptoms. They may check your thyroid (correct). They may ask about stress and life circumstances (reasonable). They may suggest talking therapy or an SSRI (logical, given the presentation).
What most GPs don’t do is connect those symptoms to hormonal fluctuation in a woman under 45, because the training model for menopause is still largely built around the 50-year-old transition. Perimenopause in women in their late 30s and early 40s, presenting primarily as mood and sleep changes with periods that are still broadly regular, falls outside the diagnostic pattern most doctors have been trained to look for.
This is not negligence. It is a knowledge gap, a significant one, documented extensively in the clinical literature on perimenopause, but not yet systematically corrected in medical training. In one 2025 national survey, only 15% of women felt adequately informed about perimenopause when their symptoms began, and fewer than half said a provider had ever raised the topic with them.
The FSH testing problem: why ‘normal’ results mean less than you think
If your doctor ordered hormone tests and the results came back normal, here is what you need to understand about that result.
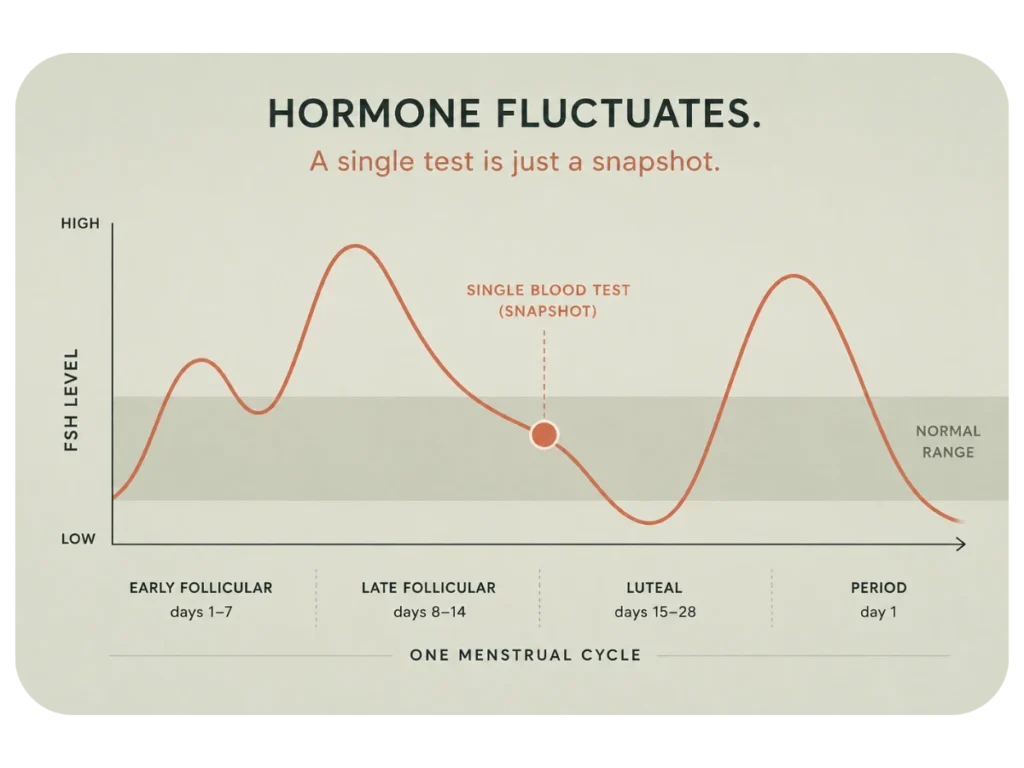
Standard hormone testing measures FSH (follicle-stimulating hormone) and estradiol. In early perimenopause, both of these fluctuate dramatically, sometimes within the same week, sometimes within days of each other. A blood test taken at the wrong point in the cycle can show a perfectly normal FSH even when you are well into the hormonal fluctuation of early perimenopause.
What ‘normal FSH’ means, and doesn’t mean: It means your FSH was within the reference range on the day the blood was drawn. It does not mean you are not in perimenopause. It does not mean your hormones are not fluctuating. It does not mean your symptoms are not hormonal. Many specialist menopause practitioners diagnose early perimenopause on symptoms and pattern, not on a single hormone number. A normal FSH result is one data point, not a verdict.
This is exactly why tracking hormone levels across a full cycle, rather than a single blood draw, gives a far more complete picture. A specialist wants to see the curve of your hormones over time, not a single snapshot. A snapshot can look normal even when the pattern isn’t. We’ll come to the tools for that shortly.
The age bias: ‘you’re too young’ is a training artifact, not a fact
The documented clinical onset range for perimenopause begins in the late 30s. ‘You’re too young’ is not based on current evidence. It is based on an outdated model that still places the menopause transition firmly in the early 50s.
If you have been told you are too young, you have encountered a knowledge gap in your doctor’s training, not a truth about your body. You are allowed to push back. You are allowed to ask for a referral. You are allowed to seek a second opinion from a NAMS-certified menopause specialist, which is the credential that specifically indicates expertise in exactly this kind of early-transition presentation.
Can You Have Both? Perimenopause Anxiety AND an Anxiety Disorder
Yes. This is worth addressing directly, because many women reading this will have been treated for anxiety for years, and are wondering whether that treatment was wrong, or whether there are now two things happening at once.
Both can be true simultaneously. Perimenopause can exacerbate a pre-existing anxiety disorder significantly. And the hormonal fluctuations of early perimenopause can generate anxiety symptoms in women who have never experienced anxiety before. Neither rules out the other.
What matters is whether the hormonal component is being identified and treated, not just the anxiety. A woman who has primary GAD and is entering perimenopause may need both the psychological treatment she’s already receiving and hormonal support, and getting one without the other means her treatment is incomplete.
If you have been in treatment for anxiety and it has worked reasonably well for years and then suddenly stopped working, or worked less well, without any change in your psychological circumstances, that shift is worth investigating hormonally. Perimenopause affecting the same neurotransmitters that your anxiety treatment targets is a plausible explanation, and it’s treatable.
How to Tell the Difference: The Practical Self-Assessment
This is not a diagnostic tool. Only a qualified clinician can diagnose perimenopause or an anxiety disorder, and you should talk to a doctor who will actually listen to you. What this is: a structured way of observing your own patterns over one menstrual cycle, so you arrive at that appointment with data instead of just a description of how you feel.
Data changes conversations. ‘I’ve been anxious’ is something a doctor can attribute to stress. ‘My anxiety spikes in the 7-10 days before my period, I wake between 3 and 4am without anxious thoughts, and my periods have become heavier and less predictable over the past 18 months’ is a clinical pattern that is much harder to dismiss.
The 12-question pattern check: complete over one full cycle
Category A: Pattern questions, looking for the cyclical signature
These questions look for the hallmark of hormone-driven symptoms: a pattern that tracks with your menstrual cycle.
A1. Do your anxiety, irritability, or low mood get noticeably worse in the 7-10 days before your period starts?
A2. Have your periods changed in the past 12-24 months: heavier, lighter, closer together, further apart, or less predictable?
A3. Do you wake between 2 and 4am without a specific worry keeping you awake, just wide awake, sometimes with a racing heart?
A4. Did these symptoms arrive or intensify within the last 12-36 months, without a clear life trigger that explains them?
Category B: Mechanism questions, physical vs thought-driven
These questions target the quality of the symptoms rather than the pattern, specifically whether the anxiety is being generated physically or mentally.
B1. Does your anxiety feel physically generated, a bodily state you’re trying to explain, rather than caused by specific worried thoughts?
B2. Do you experience heart palpitations or heat sensations that occur at rest or at night, not specifically during anxious moments?
B3. Does your mood shift seem to have no external trigger? It just arrives, and sometimes just lifts, without corresponding to events?
B4. Do you notice any improvement in your symptoms in the first week after your period starts?
Category C: Ruling out other causes
Before attributing everything to perimenopause, it’s worth making sure other common causes have been excluded.
C1. Has your doctor checked your thyroid function (TSH) recently? Thyroid imbalance produces almost identical symptoms and is common in women in this age range.
C2. Has a blood panel excluded B12 deficiency, iron-deficiency anemia, and vitamin D deficiency? All three can produce fatigue, mood changes, and brain-fog-like cognitive symptoms.
C3. Are you currently taking SSRIs, hormonal contraceptives, or beta blockers? All of these can alter mood, sleep, and anxiety in ways that overlap with perimenopause symptoms.
C4. Have you been under significant unusual stress in the past 1-2 years? This might explain a portion of what you’re experiencing, without explaining all of it.
Download the 12-question pattern check (PDF)
How to read your answers: 3 or more ‘yes’ responses in Category A indicate a strong cyclical, potentially hormonal pattern. 2 or more ‘yes’ responses in Category B mean symptoms are likely physiological rather than thought-driven. Any ‘yes’ in Category C means confirm that cause is excluded before focusing on perimenopause. This checklist is not diagnostic. It is a structure for observing and reporting patterns, which is exactly what your next medical conversation needs.
‘But My Tests Came Back Normal.’ What to Do When the System Has Let You Down
You tracked your symptoms. You went back to your doctor. You described the cyclical pattern, the waking without worry, the period changes. Your FSH came back within range. And you were, once again, told you’re fine.
You are not fine. You know you are not fine. And ‘normal FSH’ is not the same as ‘not in perimenopause.’ We’ve established that. So here’s what the next step actually is. It’s about getting hormone data you own, that tracks across your cycle, instead of a single point-in-time blood draw.
Why tracking across your cycle matters more than a single blood test

The core problem with standard hormone testing for perimenopause in your late 30s is the single-snapshot limitation. Hormones in early perimenopause fluctuate dramatically. FSH can be within range one week and elevated the next. Estrogen can be normal on Monday and dysregulated by Thursday. A single blood draw captures a moment, not a pattern.
What clinicians who specialize in early perimenopause diagnosis actually want to see is the pattern across at least one, ideally two, full cycles. That pattern, the shape of your hormone curve, not a single point on it, is what they use to identify whether fluctuation is happening and what stage of the transition you’re in.
At-home hormone monitoring has become sufficiently accurate to give you this data. Not to replace clinical care, but to give you something concrete to bring to your next appointment, or to your first appointment with a specialist who will actually listen.
The at-home hormone test built for this exact situation
Mira’s Menopause Transitions Kit is the option we’d recommend for women in this specific situation: already dismissed by their GP, wanting real data across a full cycle, and needing something more than a single FSH panel.
Unlike a mail-in blood spot test, Mira monitors four key hormones (FSH, LH, estrogen (E3G), and progesterone (PdG)) across multiple days of your cycle. You test with a small wand at home, the device reads your hormone concentrations in 16 minutes, and the app tracks the pattern over weeks and months. That’s a hormone curve. That’s the thing a specialist can actually interpret.
Mira Hormone Monitor: Menopause Transitions Kit (recommended). From around $179. Tracks FSH, LH, estrogen, and progesterone across your full cycle. Designed for women 35-60 navigating perimenopause, with lab-grade fluorescent technology and exportable hormone reports you can bring to your appointment. Includes the Menopause Mode in the Mira app, which identifies your transition stage based on your personal data, not a population average.
A few honest notes before you decide: Mira is a monitoring device, not a diagnostic tool. It will show you your hormone pattern, but a qualified clinician still needs to interpret that pattern in context. And it requires consistent daily testing across your cycle to give meaningful data. This is not a one-time test. If you’re looking for a one-time snapshot to start the conversation, the option below is the right fit instead.
The one-time option: Everlywell Perimenopause Test
If you want a starting point before committing to ongoing monitoring, Everlywell’s Perimenopause Test is a mail-in finger-prick blood panel that measures FSH, LH, and estradiol. Results arrive in around 5-8 days after the lab receives your sample, reviewed by a physician, and are presented in a clear results report.
It’s a single snapshot, not a pattern across your cycle, so it has the same limitation as your GP’s blood test if timed incorrectly. But used strategically (ideally in the early follicular phase, days 3-5 of your cycle), it gives you a baseline and physician-reviewed context, which is often enough to kickstart a more useful medical conversation.
Everlywell Perimenopause Test (good starting point). Around $99. A one-time finger-prick panel with results in about 5-8 days. Measures FSH, LH, and estradiol, processed in CLIA-certified labs with physician-reviewed results. No appointment, no waiting room, FSA/HSA eligible. A solid option if you want a documented hormone baseline before your next appointment, or before committing to ongoing cycle tracking.
Want the full picture before you buy? We compared the main at-home options side by side (what each measures, what they cost, and which one to skip) in our complete guide to at-home hormone tests for perimenopause.
Perimenopause Anxiety Treatment: Your Next Three Steps
You’ve read the symptom patterns. You’ve done the self-assessment. You think, or you’re starting to think, that what you’ve been told is anxiety may actually be something hormonal. Here’s the path forward. Not overwhelming. Not a 20-item plan. Three steps, in order.
Step 1. Track your symptoms across one full cycle before your next appointment. Thirty days. Map your anxiety, mood, sleep, and energy against your cycle days. Note when symptoms are better, when they’re worse, whether they follow a pattern relative to your period. This is the data that changes the conversation from ‘I feel anxious’ to ‘I have a cyclical pattern of anxiety that spikes in my luteal phase and resolves after my period starts.’ One is a symptom report. The other is a clinical pattern. Download our free 30-Day Perimenopause Symptom Tracker.
Step 2. Get hormone data you control, ideally tracking across your cycle. If your single-point blood test has come back normal and you’re still not getting answers, at-home hormone monitoring gives you the pattern data a specialist can actually use. Mira’s Menopause Transitions Kit tracks four hormones across multiple days. Everlywell’s Perimenopause Test gives you a one-time snapshot if you want to start there. Either way, arriving at your next appointment with documented hormone data, not just symptoms, shifts the dynamic significantly.
Step 3. Find a clinician who specializes in perimenopause, not just a GP who will listen. Your GP’s training may simply not include early perimenopause presentation. That’s not a character flaw. It’s a structural gap. If you’ve been dismissed twice, the solution is not to be more persuasive in your current appointment. It’s to find a different kind of specialist. A NAMS-certified menopause practitioner is the specific credential to look for. Telehealth options like Midi, Alloy, and Winona now make this accessible without a referral. See our full comparison of perimenopause telehealth providers.
You Were Right to Keep Looking
You described a set of symptoms. A doctor, maybe several doctors, gave you a diagnosis. And you left each appointment with a quiet sense that the explanation didn’t quite account for everything you were experiencing. And you kept looking.
That instinct was correct.
If you’ve been Googling ‘perimenopause vs anxiety’ trying to work out which one fits your experience, that question itself is the right one. Perimenopause anxiety in women in their late 30s and early 40s is real, documented, and systematically under-diagnosed. The psychological symptoms that arrive before hot flashes are real. The hormone imbalance anxiety connection (the fluctuating estrogen and progesterone disrupting the same neurotransmitters that regulate mood) is real. The feeling that something has shifted in your body and your mind is scrambling to explain it is a clinically meaningful observation, not hypochondria.
The next step is data. Not another appointment where you leave feeling dismissed. Actual hormone data across your cycle, and a clinical pattern you’ve tracked yourself, so that the next conversation is about evidence rather than persuasion.
Track What’s Happening — Free 30-Day Perimenopause Symptom Tracker
Thirty days of symptom data, mapped to your cycle, formatted to bring to your doctor. Five minutes a day. At the end of 30 days, you’ll have a pattern, not just a feeling.