

This article contains affiliate links. If you purchase through our links, we may earn a small commission at no extra cost to you. This does not affect our editorial recommendations.
It’s late. You’re tired, bone-tired in a way that sleep doesn’t fix anymore, and you’re Googling something you’re not entirely sure you’re allowed to Google yet. Because perimenopause is for women in their 50s, right? Older than you.
Except something is wrong. Something has been wrong for a while. And ‘stress’ stopped being a good enough answer around the time your doctor said it for the third time.
You’re not too young. You’re not imagining it. If you’re recognizing these early signs of perimenopause in your 30s, this article was written for you. For the experience you’ve been trying to name.
Everything here is drawn from peer-reviewed clinical research and the patterns thousands of women describe living through. You deserve more than another wellness blog’s take on this.
This article isn’t a checklist of hot flash symptoms. If you’re in your late 30s or early 40s, hot flashes are probably not what’s bringing you here. They’re often not what comes first either. What comes first is subtler, stranger, and harder to name. What comes first is probably what you’ve already been experiencing.
And the first thing we need to talk about isn’t what you think.
First: The Early Signs of Perimenopause in Your 30s That Have Nothing to Do With Hot Flashes
Here is the thing nobody tells you. It’s the single most important fact in this entire piece:
| For many women, the first signs of perimenopause in your 30s are psychological. Not physical. |
The anxiety that showed up out of nowhere. The moods that feel outsized for the situation. The brain fog that makes you feel like you’re watching your own life through glass. The depression that arrived without a clear reason. These are not stress responses. They are not personality changes. They are, in many cases, the earliest signs that your hormones have begun to shift.
This is documented, not anecdotal. A 2025 study published in npj Women’s Health found that psychological symptoms not only precede physical ones in perimenopause. They tend to peak between ages 41 and 45. The window your doctor is not watching.
The psychological symptoms that come first and why they arrive before anything else
Estrogen is not just a reproductive hormone. It directly influences serotonin, dopamine, and norepinephrine: the neurotransmitters that regulate mood, focus, and anxiety. When estrogen begins to fluctuate in the early stages of perimenopause, these systems feel it.
Anxiety that doesn’t match your life. Not the ‘big presentation tomorrow’ kind. The kind that wakes you at 3am for no reason. The kind that sits in your chest on a perfectly ordinary Tuesday. The kind that made you wonder, seriously, whether you had developed an anxiety disorder out of nowhere.
Mood swings that feel disproportionate. You are a capable person who manages everything. And then you’re snapping at someone you love over something small and watching yourself do it and not entirely understanding why. This has a name. We’ll get to it.
Brain fog and memory gaps. Losing words mid-sentence. Walking into a room and forgetting why. Reading the same paragraph four times. Some women describe this as the most frightening symptom. Not because of tiredness, but because it feels like cognitive decline. It is not cognitive decline. It is estrogen’s effect on the hippocampus being disrupted by fluctuating hormone levels.
Depression with no clear cause. Not situational sadness that makes sense in context. A flatness. A heaviness. An absence of things that used to feel good. In perimenopausal women, this is frequently treated as primary depression, which is why nearly 40% of women seeking care for perimenopause symptoms are misdiagnosed, and more than half are treated for anxiety or panic attacks instead of what’s actually happening.
Why your doctor saw anxiety and missed the hormone connection
Here is what happened at that appointment. You described your symptoms. Your doctor heard ‘anxiety’ and ‘mood changes’ and ‘sleep problems’ and ran a completely reasonable diagnostic process. A process built for anxiety, mood changes, and sleep problems. They may have checked your thyroid. If they ordered hormone tests at all, the results probably came back ‘normal.’
And then they said: you’re under a lot of stress. You might benefit from therapy. Here’s a prescription, if you want it.
This is not negligence in most cases. It is a knowledge gap that has persisted in medical training for decades, specifically around early perimenopause presentation in women under 45. In one 2025 national survey, only 15% of women felt adequately informed about perimenopause when their symptoms began, and fewer than half said a provider had ever raised the topic with them. The information gap runs in both directions.
You are allowed to go back. You are allowed to ask a different question. We’ll give you the language to do that later in this article.
The Physical Signs That Show Up Before Hot Flashes
Now that we’ve reframed what the early signs actually look like. Not the hot-flash picture. The real picture. The physical symptoms make more sense too. Because they’re connected to the same hormonal fluctuations. They just manifest differently in your body.
Sleep falling apart: the 3am wake up nobody warned you about


This is one of the most common early physical signs. It’s also one of the most disruptive, because everything else in your life gets harder when you’re not sleeping.
The pattern is distinctive. You fall asleep fine. You wake somewhere between 2 and 4am, fully alert, often with a racing heart or a sense of unease, and you cannot get back to sleep for an hour or two. Then you wake exhausted and spend the day running on fumes.
This happens because progesterone, one of the first hormones to decline in early perimenopause, has a natural sedating effect. When progesterone begins to drop, that sedating effect decreases, and sleep architecture changes. You spend less time in deep, restorative sleep and more time cycling through lighter stages. The 3am wake-up is not insomnia in the traditional sense. It is a hormonal signature.
Night sweats can accompany this, though not always. You might feel suddenly, inexplicably overheated at 3am. Not dramatically. Not like the hot flashes you’ve seen depicted. Just warm enough to kick off the covers, just uncomfortable enough to wake you. This is vasomotor activity. It can be subtle in the early stages.
Weight creeping up despite nothing changing: What’s actually happening
If your weight has shifted, particularly around your midsection, in a way that feels different from previous fluctuations and resistant to the things that used to work, this is not a willpower failure.
As estrogen begins to decline, the body undergoes a metabolic shift. Fat storage redistributes toward the abdomen. Insulin sensitivity changes. The relationship between food, exercise, and body composition that you’ve relied on for years begins to function differently. At the same time, cortisol becomes more influential as estrogen drops, and elevated cortisol is directly associated with visceral fat accumulation.
This is not about eating more. This is about your hormonal environment changing the rules.The frustrating part is that this symptom is almost never identified as hormonal when it appears in a 38-year-old. It gets attributed to aging, to slowing metabolism, to ‘you’re not as young as you used to be.’ Which is technically true. Just not in the way it’s being said.
Irregular periods: heavier, lighter, or just weird
Your cycle has been reliably yours for two decades. You knew what to expect. And now you don’t.
Maybe your periods are heavier than they used to be, significantly so, with clotting that feels alarming. Maybe they’re lighter and shorter. Maybe the timing has shifted. Cycles that used to be 28 days are now 24, or 35. Maybe you’ve skipped one and panicked, only for it to arrive three weeks later.
All of this: the variation, the unpredictability, the periods that seem to have forgotten their own rules, is characteristic of the early perimenopause transition. As estrogen and progesterone fluctuate rather than following their previous pattern, the lining of the uterus responds differently each cycle.
This does not mean your periods will become immediately irregular. Many women in early perimenopause continue to have regular cycles for years while experiencing significant hormonal fluctuation. The fact that your period still arrives roughly on time does not rule out perimenopause.
Heart palpitations, joint pain, and the symptoms that sent you to Google
These are the symptoms that tend to generate the most frightening search sessions.
Heart palpitations: a sudden awareness of your heartbeat, a flutter, a thud, a momentary skip, are experienced by a significant portion of perimenopausal women and are directly related to estrogen’s effect on the cardiovascular system. They are almost always benign in the context of perimenopause, but alarming enough that many women end up in urgent care or the cardiologist’s office first.
Joint pain and stiffness, particularly in the hands, knees, and hips, is less commonly discussed but well documented. Estrogen has anti-inflammatory properties. As it begins to fluctuate, the joint protection it provides becomes inconsistent, and many women notice new achiness, stiffness in the morning, or joint pain that seems unrelated to exercise or injury.
Headaches, particularly new patterns of migraines, can emerge or worsen. Dry eyes, dry skin, changes in body odor. All documented perimenopause presentations. Fatigue that doesn’t respond to sleep.
The connecting thread in all of these is estrogen’s reach. It is not a reproductive hormone that happens to also affect your uterus. It is a systemic hormone with receptors throughout your entire body: your brain, your joints, your cardiovascular system, your skin, your gut. When it fluctuates, the effects are systemic.
Perimenopause or Burnout? Or Both?
This is the question that keeps most women in their late 30s from getting the right answer for years.
Because the honest answer is: it can be both. Genuinely. At the same time. And the fact that you are also burned out, exhausted, overwhelmed, stretched too thin, does not cancel out the possibility that your hormones are also shifting. These two things are not mutually exclusive, and conflating them is one of the primary ways women in this demographic get stuck.
The symptoms that look identical to burnout and the one key difference
Burnout and early perimenopause share a striking symptom overlap: fatigue, emotional dysregulation, cognitive difficulty, sleep disruption, loss of enjoyment in things that used to bring pleasure, irritability, anxiety. If you describe these symptoms to a physician who knows you’re a high-achieving woman in a demanding life stage, ‘burnout’ is the natural conclusion.
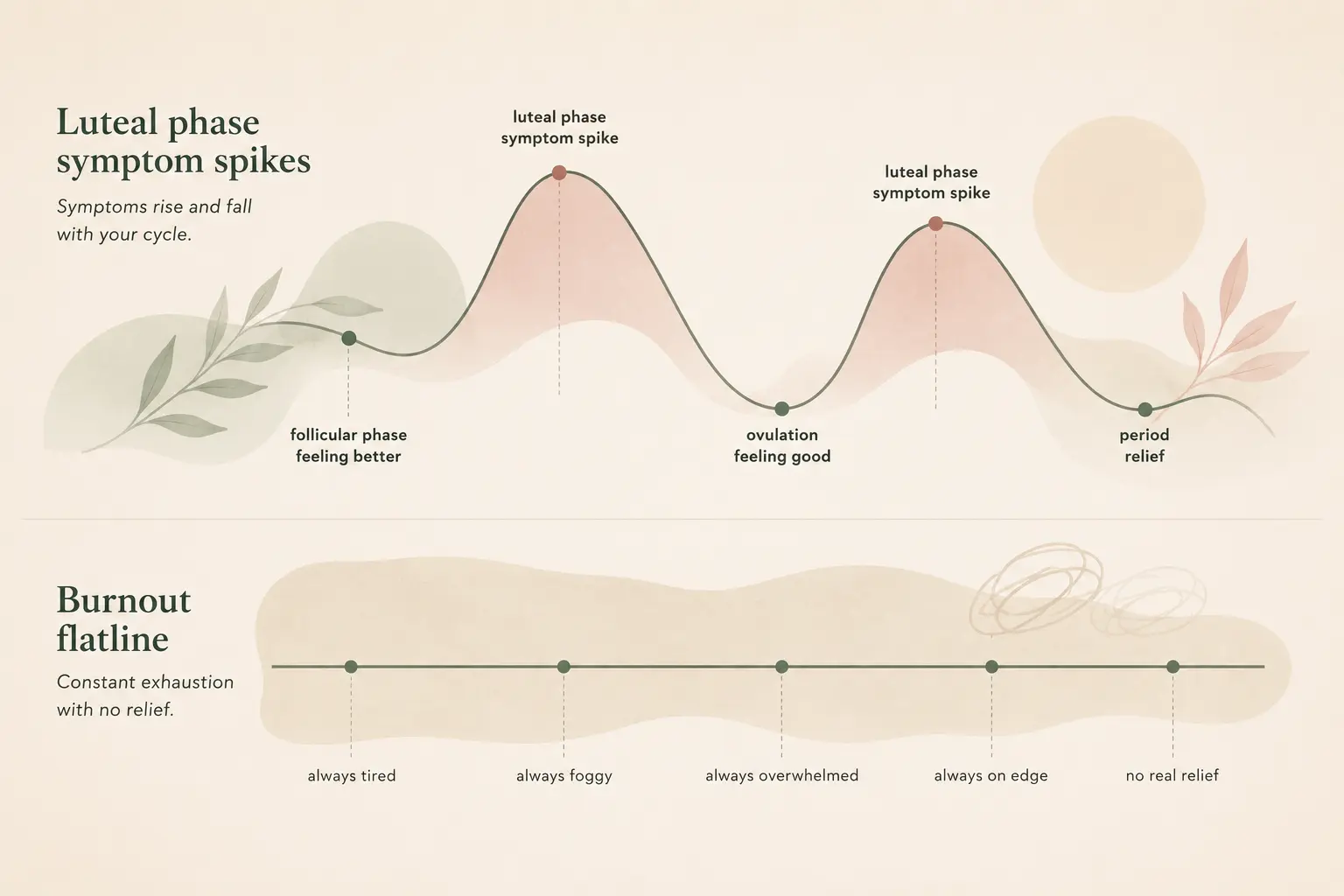
The key distinguishing feature is cyclical pattern.
Burnout tends to be relatively consistent. Bad days and slightly less bad days, but not dramatic fluctuations tied to a calendar. Perimenopause symptoms often, though not always, follow a hormonal rhythm.
The anxiety that spikes in the week before your period and settles within a few days of bleeding. The fog that descends on day 21 and lifts on day 6. The sleep that falls apart the week before your period and recovers the week after. The rage that arrives reliably in the luteal phase and then, just as reliably, recedes. If these patterns sound familiar. If you’ve noticed that you’re not consistently terrible but cyclically terrible, that is important clinical information.
Tracking your symptoms against your cycle for 30 days is not a diagnostic test. But it is the single most useful thing you can do before your next appointment. It helps with identifying a cyclical pattern and with giving your doctor something concrete to work with rather than a general description of feeling terrible.
(The free symptom tracker at the bottom of this article maps to your cycle specifically. It’s designed for exactly this.)
One group who should pay particular attention to the cyclical pattern: women who were previously diagnosed with PMDD. PMDD symptoms frequently escalate in early perimenopause. The same hormonal fluctuation that drove your luteal-phase symptoms gets amplified as estrogen begins to fluctuate more dramatically. If you’ve been managing PMDD for years and it’s suddenly worse, or responding less well to what used to help, perimenopause may be part of the picture.
What a perimenopause timeline actually looks like in your late 30s
The average age of the final menstrual period is 51. But perimenopause, the transition that precedes it, can begin 4 to 10 years before that last period. Which means for many women, the transition is well underway in their late 30s.
This is not unusual. It is not rare. It is the normal range.
What makes it feel unusual is that the cultural story of menopause starts at 50 and ends at ‘hot flashes.’ The transition that happens in your 30s and early 40s doesn’t have a cultural narrative yet. There are no books at the doctor’s office about it. There are very few physicians who think to mention it. You are living through something real that the medical establishment is only beginning to take seriously.
Am I Too Young for This? (No. Here’s the Actual Data.)
Here are the numbers that should have been on the wall of your doctor’s waiting room.
You are not too young. That’s not reassurance. That’s clinical fact.
The documented onset range for perimenopause begins in the late 30s. The ‘you’re too young’ response you may have received is not based on current evidence. It’s based on a model of menopause that assumes a sharp transition in the early 50s, when the reality is a years-long hormonal fluctuation that begins much earlier.
When perimenopause actually starts and why 38 is not unusual
Perimenopause does not begin on a specific birthday. It begins when the ovaries start producing less consistent levels of estrogen and progesterone. This is a process that unfolds gradually, often over years, with fluctuations rather than a steady decline.
For some women the earliest shifts show up in their mid-to-late 30s. For some it begins at 44. The average is somewhere in the early-to-mid 40s, but the range is wide and the early end of that range is more common than most women are told.
What makes early perimenopause particularly difficult to identify is that it often begins while your periods are still regular, or nearly so. Many women in early perimenopause continue to cycle, and even to ovulate, while experiencing significant hormonal fluctuation between cycles. The absence of irregular periods does not mean you are not in perimenopause.
Why your tests keep coming back normal — and what that actually means
This one matters, because it is responsible for a huge proportion of the dismissal women in their late 30s experience.
The standard hormone tests ordered to ‘check for menopause’ measure FSH (follicle-stimulating hormone) and estradiol. In early perimenopause, these levels fluctuate dramatically, sometimes within the same week.
A test taken at the wrong point in the cycle will show a normal result. A test taken a week later might show something entirely different. This is not a flaw in the testing. It’s a feature of early perimenopause itself. The fluctuation is the condition.
To make this concrete: a woman in early perimenopause might have an FSH of 8 on cycle day 3 and an FSH of 18 on cycle day 10. Both are technically within a ‘normal’ range, but the variation itself is the signal. A single draw that catches a low-fluctuation day tells your doctor almost nothing.
Many specialist menopause practitioners do not rely primarily on hormone levels for diagnosis in this stage. They treat symptoms. They listen to the pattern. They understand that a woman who describes 14 months of cyclical anxiety, disrupted sleep, and changing periods with normal FSH results is not ‘fine’. She is in early perimenopause with a currently normal FSH result.
This distinction, between a test result and a clinical picture, is one of the most important things to understand going into any perimenopause diagnosis conversation.
What’s Actually Happening to You: The Breakdown Nobody Shows You
This is the version of the symptom picture that maps to your real experience. Not the version in the pamphlet in the waiting room.
What you were told: Stress, work pressure, ‘you have a lot going on.’
What it might actually be: Estrogen fluctuation affecting serotonin and the HPA axis.
What you were told: Too much caffeine, screen time, stress.
What it might actually be: Early progesterone decline altering sleep architecture.
What you were told: Depression, burnout, ‘you seem stressed.’
What it might actually be: Estrogen-serotonin disruption. Documented. Treatable. this block. You can use this space for describing your block.
What you were told: Overwork, burnout, ‘just tired.’
What it might actually be: Estrogen effects on hippocampal function and neurotransmission.
What you were told: Slower metabolism, ‘you’re getting older.’
What it might actually be: Cortisol-estrogen interaction, insulin sensitivity shift.
What you were told: Anxiety, ‘let’s check your heart.’
What it might actually be: Vasomotor symptoms. An early perimenopause presentation.
What you were told: Overuse, aging, ‘just take ibuprofen.’
What it might actually be: Estrogen’s anti-inflammatory role becoming inconsistent.
If you read through the information above and feel the particular relief of recognition. Of seeing your experience described accurately for the first time. That recognition is the point. You are not making this up. You are not catastrophizing. You are living through something real that has a name, a mechanism, and a path forward.
The ‘I’m Not Getting Taken Seriously’ Problem
We need to talk about this directly, because it is not in your head.
The dismissal is real. The statistics bear it out. The experience of being told ‘you’re too young’ or ‘your tests are normal’ or ‘it’s probably just stress’ when you know. When you know your own body after four decades in it. When you know that something is wrong. That is not hypochondria. It is a healthcare gap that disproportionately affects women in this exact age bracket, presenting with exactly these symptoms.
You are not the problem. The system is not calibrated for you yet.
The language that actually gets you heard
You do not have to arrive claiming a diagnosis. What you can do is describe a clinical pattern with specificity. That is a different conversation entirely.
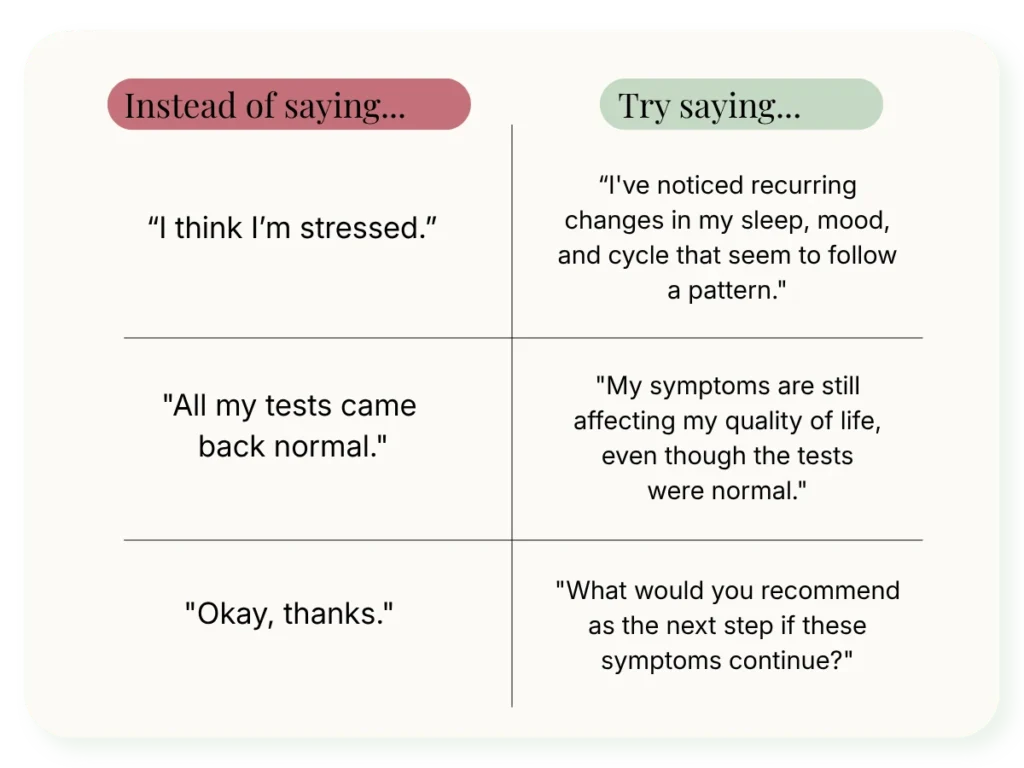
You are not asking for permission to have this experience. You are asking for the clinical conversation your symptoms warrant.
For a full guide to this conversation. What to bring, what to ask for, and what to do if you’re still dismissed. Read how to talk to your doctor about perimenopause without being dismissed.
So What Do You Actually Do Next?
Understanding what’s happening is the first step. Here are three concrete paths forward. Not overwhelming. Not prescriptive. Just the next move for wherever you are right now.
Step one: Track your symptoms before your next appointment
Thirty days. Your cycle. Write it down. Or use the free 30-day symptom tracker below, which is specifically designed for this.
When you arrive at an appointment with a month of charted symptoms mapped against your cycle, you are no longer asking your doctor to believe your subjective experience. You are presenting data. The conversation changes.
The tracker maps the specific symptoms of early perimenopause, including the psychological ones, against cycle days. It has a ‘bring to your appointment’ column designed to be printed. It takes five minutes a day and 30 days of it can change the quality of every medical conversation you have from here forward.
Step two: Consider getting hormone data before your next appointment
At-home hormone testing has become significantly more sophisticated in the last few years. Rather than a single blood draw, at-home hormone monitors now allow you to track levels over multiple days. This gives a much more complete picture of the fluctuation pattern than a one-time lab result.
This isn’t a replacement for clinical care. But it can give you real data, a hormone pattern over time, to bring to an appointment. For a full comparison of the main options, what each one measures, and which situations they’re best suited for: the best at-home hormone tests for perimenopause, compared.
Step three: Know that specialist care for this exists and it’s now accessible
If your GP continues to dismiss you, that is not the end of the road. It is the end of one road.
There are now perimenopause specialists you can see online. Women’s health providers who focus specifically on this transition, who understand the early presentation, who do not require a ‘normal’ FSH result to take your symptoms seriously. They prescribe. They follow up. They adjust.
This kind of care exists, and it’s available without leaving your house. When you’re ready to explore it, we’ve done a full comparison of the main providers, what each costs, and which situations they’re best suited for. See the best telehealth for perimenopause: our 2026 comparison.
You Were Right to Keep Looking
You are in your late 30s, something is wrong, and you have been told. Told by people who were supposed to know. That you are too young, too stressed, too much. You believed them, partly, because they were the experts. And then you kept looking anyway, because your body kept telling you something they weren’t hearing.
That instinct was correct.
Perimenopause in your late 30s and early 40s is real. The psychological symptoms that arrive before the physical ones are real. The hormone fluctuations that don’t show up clearly on a single blood test are real. The dismissal at the doctor’s office is real, and it is a gap in the system. Not a reflection of whether your experience is valid.
And perimenopause, once recognized, is treatable. You don’t have to white-knuckle through this. The next move is tracking what’s happening. So you have something concrete to bring to the conversation.
Track What’s Happening — Free 30-Day Perimenopause Symptom Tracker
Thirty days of symptom data, mapped to your cycle, formatted to bring to your doctor. Five minutes a day. At the end of 30 days, you’ll have a pattern, not just a feeling.
Ready to get actual hormone data? Our guide to at-home hormone testing walks through the main options and which makes most sense depending on where you are in the process.
This article is for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare provider if you are experiencing symptoms that concern you.